
Thyroid
The thyroid is a relatively small organ, lying against and around the larynx and trachea. Female thyroid glands weigh up to 18 g, male ones up to 25 g.
The thyroid gland produces, among others, the two vital hormones T3 (triiodthyronine) and T4 (thyroxine). These thyroid hormones regulate important functions in the body:
The whole metabolism, heart and circulation, stomach and intestines, nerves and muscles
The thyroid hormones also affect personality and mental well-being, sexuality and fertility and the growth of skin, hair and nails.
In infants and adolescents, the thyroid gland plays a very special role. It controls the entire physical and mental development.
The work of the thyroid gland is controlled by the pituitary gland (hypophysis): the thyroid stimulating hormone (TSH), which stimulates the hormone secretion of the thyroid gland, is produced there.
The thyroid gland needs iodine as an important element for the production of its hormones. Normally, an adult needs about 150-200 micrograms of this essential trace element daily in order to supply the thyroid with a sufficient amount of iodine.
Depending on age and personal situation iodine requirements may also be higher, e.g. during pregnancy and lactation.
An iodine deficiency leads to changes in the thyroid, e.g. unusual growth, nodulation and malfunction.
The iodine uptake in the thyroid gland can be increased by consumption of iodized foods (e.g. fish), use of iodized salt or intake of iodine tablets.
The intake of iodine in the form of tablets is particularly important during pregnancy, lactation and adolescence (between 6 and 18 years), because in these cases the iodine intake by food is often insufficient in Germany. The intake of iodine tablets should however always take place after consultation with the doctor.
Diseases of the Thyroid can manifest themselves in several ways:
- Physical characteristics: growth of the thyroid gland, which then leads to the development of a goiter and/or nodules.
- Disruption of hormone production: the thyroid gland is over-active (hyperthyroidism) or under-active (hypothyroidism)
- Pain or feeling of obstruction in the throat in the context of inflammatory changes of the thyroid gland
- The latest survey of more than 150,000 people in Germany has shown that about one in three adults has such changes of the thyroid, in patients older than 45 years even every second.
Examination of the Thyroid
A step-by-step approach is usually applied in the diagnosis of the thyroid gland: at first the medical history (anamnesis) is collected, followed by physical and ultrasound examination of the thyroid gland as well as different laboratory tests and functional scintigraphy depending on the results so far.
1. Collection of medical history and complaints
2. Physical examination (palpation of the neck region)
3. Ultrasound examination (sonography) and, where appropriate, real-time elastography
4. Scintigraphy (functional and/or MIBI scintigraphy)
5. If appropriate, fine-needle aspiration
6. Immunological laboratory tests
7. Proliferation markers or growth factors
From the synopsis of all results an as accurate as possible diagnosis can then be made and an individual therapy plan that is tailored to the patient can be created. Since our practice is specialized for a long time on the diagnosis and treatment of thyroid diseases, the treatment of our patients is carried out in consideration of all known effects and influences on this important organ.
In our practice, each patient receives an individual thyroid pass – similar to a vaccination certificate. This includes all appointments and your current medication. The thyroid pass helps you and the treating physician to recognize your thyroid status and the current medication.
Examination of the Thyroid in detail
1. Collection of medical history and complaints

Ultrasound examination of the thyroid
It is important for us to get to know medically relevant information of our patients before an examination and report. This includes former diseases, any current complaints and medication. Through a short questionnaire and the physician-patient consultation we get a good overview and we can take an integrated approach to diagnosis and therapy.
2. Physical examination (palpation of the neck region)
This examination serves in particular to palpate nodules and indurations of the thyroid gland and to compare the thyroid gland with its typical structure.
3. Ultrasound examination (sonography) and, where appropriate, real-time elastography
This examination serves to visually capture structure, size, possible nodules and circulation of the thyroid gland.
Depending on the case, the real-time elastography – one of the most modern methods of examination to clarify the consistency of nodes – is used. In this case, the elasticity of the nodes is examined. Hardened tissue should be further examined. On the other side, soft, elastic tissue is indicative for benign changes in the thyroid.
Thyroid overactivity, a so-called hot nodule
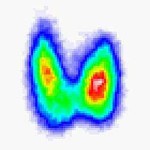
4. Thyroid scintigraphy
For this examination specific radioactive substances (so called radionuclides) are used. The most commonly used substance is radioactive technetium-99m, which is similar to the chemical element iodine. This is injected into the patient’s vein in a minimal amount and then accumulates in the thyroid. About 15 minutes later, images can then be made by the metabolic activity of the thyroid gland. An overactive thyroid (hyperthyroidism) or an acute thyroiditis can be detected with this examination.
It also serves as proof for hot and cold thyroid nodules. Hot nodes can cause hyperthyroidism, cold nodes can degenerate into the malignant form in rare cases (3-5%) and should be evaluated further.
After the examination, the doctor gets an image by which he evaluates the intensity of thyroid function as well as the location and activity of nodes.
Radiation exposure during thyroid scintigraphy is classified as very low or negligible. It is equivalent to a small fraction of the annual natural radiation exposure on Earth. The administered radionuclide is stored in the thyroid only for a short time and then rapidly excreted through the urinary tract.
MIBI scintigraphy
The MIBI scintigraphy is used for further diagnosis of so-called cold thyroid nodes. If a cold node displays conspicuously in the MIBI scintigraphy, the probability of malignancy will increase to 15-20% according to the available data. In an inconspicuous MIBI scintigraphy, however, the risk for malignancy is far below 1%. In this case, regular supervision by a specialist is sufficient.
5. Fine-needle aspiration
In case of suspect thyroid nodes, a very thin needle is guided into the thyroid nodule and a small sampling of cells is aspirated into the needle. Then, a pathologist evaluates the sample for malignancy. Combined with the previous examinations the tumor suspicion can be contained and a basis for further treatment can be created. Since we have many years of experience with fine-needle aspiration, we can assess the indications very good. The fine-needle aspiration is the best technique for detecting or ruling out the presence of cancer.
6. Immunological laboratory tests:
Nowadays extremely reliable laboratory tests are available for the diagnosis of thyroid function. These are performed as so-called immunological examinations by our specialized laboratory.
Essentially, it involves the determination of the thyroid hormones T3, T4 and the messenger of pituitary (TSH). Depending on the results a determination of the proliferation marker TG and a determination of tumor markers, such as Calcitonin can follow. Further examinations performed by our laboratory include: vitamin D, parathyroid hormone, ferritin and PSA.
For patients who live farther away or who just want a check-up blood test, the family doctor may also send a blood test to our specialized laboratory. Here, the diagnosis described above takes place. Then we will send the results to your doctor.
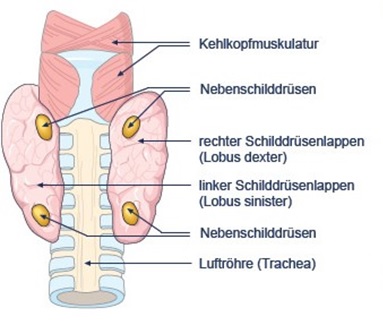
Anatomy of the thyroid